By Bela Koganti
~ 6 minutes
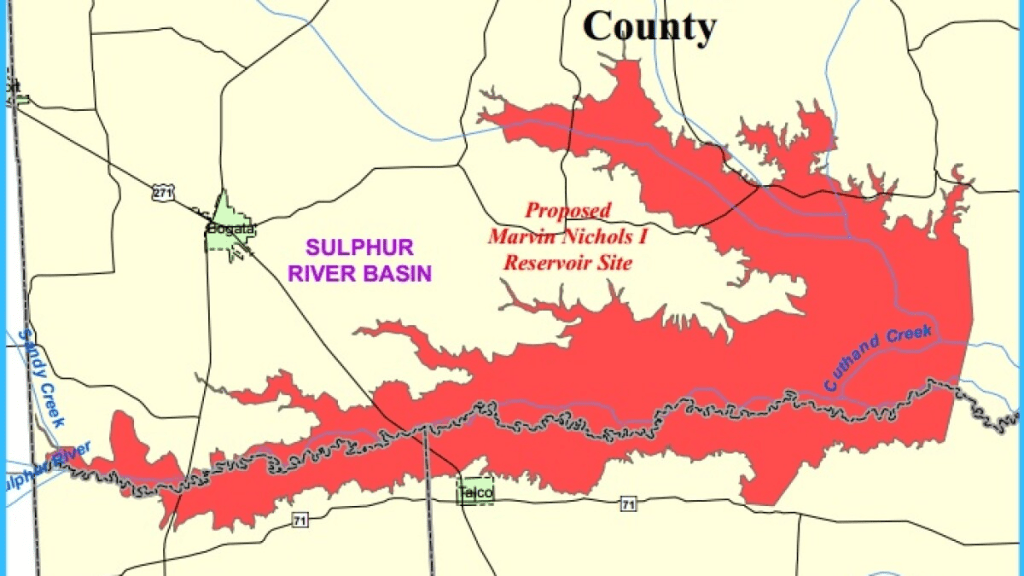
The proposed Marvin Nichols Reservoir, which would occupy over 72,000 acres in Northeast Texas, has been in the works since 1968. However, with Texas’ more-imminent-than-ever water crisis, it’s recently gained more and more traction— and just as much controversy.
What is it?
The proposed Marvin Nichols Reservoir would occupy the Sulphur River Basin and supply drinking water to the Dallas-Fort Worth area. With a plethora of available water from the basin and a low estimated water cost, the reservoir first appeared in Texas’ 1968 State Water Plan as the Naples Reservoir; then, it was proposed in the 1984, 1990, and 1997 state water plans as the Marvin Nichols Reservoir. In 1997, the 75th Texas Legislature passed Senate Bill 1, which divided Texas into 16 regions with local representatives to develop water plans.
Since then, renditions of the reservoir have been recommended in eleven regional and state water plans. While the Texas Legislature designated the reservoir site as a
“Site of unique value for the construction of a reservoir.”
In 2007, the Region D Regional Water Planning Group voted against it due to predicted negative impacts on agricultural, timber, and natural resources, as well as on local economies.
Why’s it taking so long?
First of all, it can take at least 15-20 years to receive a permit for a new lake or reservoir. The reservoir didn’t make it into the State Water Plan (under the name Marvin Nichols) until 1984, and, by 2001 (17 years later), the project was facing strong pushback from northeast Texans.
While the 2021 Region C Regional Water Plan and the 2022 State Water Plan believe the reservoir should be ready by 2050, the Bois d’Arc Lake reservoir, another controversial and large project, took just 18 years to implement. Well, we already passed the 18 year mark—24 years ago! Regional Texas water planners stress that these projects must be operational in a timely manner. In other words, they need to happen before shortages occur- not after a drought is already underway.
So, we can expect a 2050 completion unless a future water plan indicates otherwise.
What’s happening with Texas’ water crisis?
But why do we even need the reservoir in the first place? I mean, we’re obviously running out of water, but here’s why. Texas’ Region C, made up of Arlington, Carrollton, Dallas, Denton, Fort Worth, Frisco, Garland, Irving, Mckinney, Plano, Richardson, and Frisco, is rapidly growing in population. It’s predicted to grow by nearly 6,000,000 people from 2030 to 2080, and with more people comes more water demand, which would increase by around 1,000,000 acre-feet by 2080. Even with conservation tactics outlined in the Region C Water Plan, Region C would still lack around 1,000,000 acre-feet per year.
For example, Fort Worth plans to use more wastewater, so it needs to expand its water treatment plants to treat nearly 830,000,000 gallons of water per day by 2080. However, around ⅓ of the water would have to come from new reservoirs, and that’s where Marvin Nichols comes in. Of course, it would not only supply water to Fort Worth—many cities in region C likely have similar plans for Marvin Nichols.
How will Texans be affected? What’s the controversy?
Alright, let’s get to the downsides. Although the reservoir would help some of Texas’ most populous cities, the Region C crew, it would destroy around 72,000 acres of rural land in northeast Texas through flooding. And that means wetlands destroyed, jobs gone, and history killed.
Bottomland hardwood forests are Texas’ most biologically diverse ecosystems; however, from the nineteenth century to now, only ¼ of East Texas’ bottomland hardwood forests still stand. But guess what—they make up 30,000 of the 72,000 acres that Marvin Nichols plans to destroy. Plus, because the forests house so many different animal species, the reservoir would endanger wildlife already threatened in Texas, like black bears.
And since Marvin Nichols’ construction would flood so much working land, local farmers, loggers, ranchers, and livestock ranchers would very-likely lose their jobs. School districts would be wiped, Native American historical sites and family cemeteries would be destroyed, and families who’ve lived on the land for centuries would be kicked out.
Although the aforementioned Region C Water Plan tactics aren’t quite enough, if Region C goes above the conservation levels it outlines, then it could save the entirety of the water that Marvin Nichols would provide.
So, the reservoir’s proposal raises a debate of the merits of destroying livelihoods, habitats, and history to supply even more water to some of Texas’ most populated and water-consuming cities.
Is the reservoir really the best solution?
Although water costs are estimated to be relatively low once the reservoir is built, the construction of Marvin Nichols has been estimated to cost seven-billion dollars. Yup, $7,000,000,000. That’s around $97,222 per acre. To revisit our earlier comparison, the Bois d’Arc Lake reservoir cost around $1,600,000,000 for 16,640 acres—that’s about $96,154 per acre. Both reservoirs are incredibly expensive, but one has passed and the other hasn’t.
Let’s look at the cost of the Region C Water Plan’s conservation tactics. (Table from Bryan McMath’s Marvin Nichols Reservoir Project Feasibility Review)
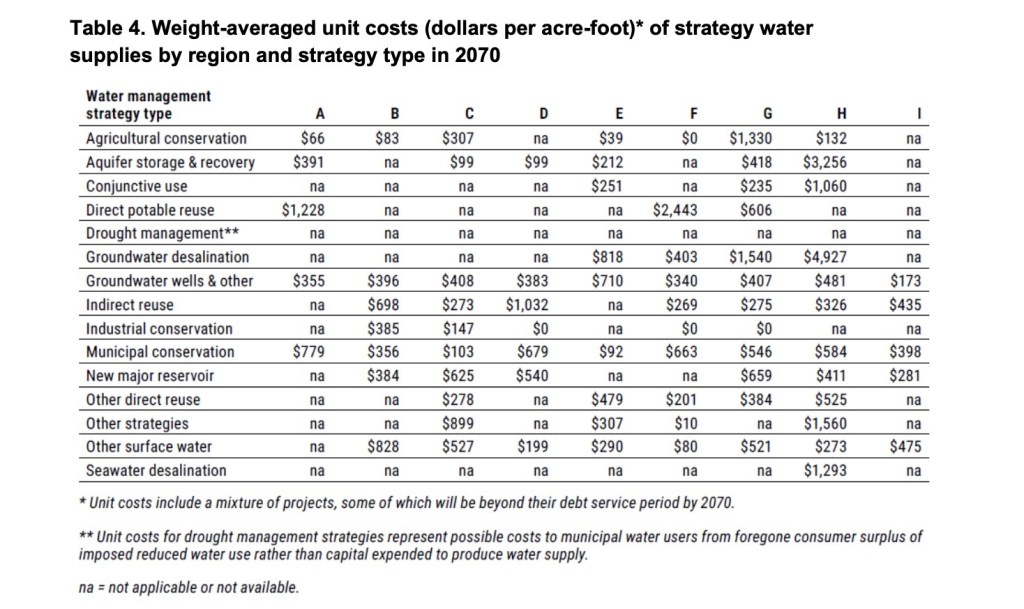
For Region C, every tactic costs immensely less than Marvin Nichols. Even by using all the tactics together, water for Region C would cost just $3,666 per acre-foot, a sharp decrease from Marvin Nichols’ construction asking for $97,222 per acre. And although only doing these tactics would leave Region C deficient of 1,000,000 acre-feet of water per year, citizens could use the strategies more aggressively with the surplus of money to fix the lack.
Marvin Nichols is not the only solution to Region C’s drinking water shortage, and it’s certainly not the best one. Let’s save the people, animals, habitats, homes, jobs, and history living in northeast Texas, and let’s do so by speaking up. If the project hadn’t received so much pushback in the early 2000s, it very well could have already been implemented or be even closer to implementation. So, we must continue to push back because our voices—Region C’s and Regions A through Z’s alike—are the most powerful tools we have to stop Marvin Nichols.