Drugs are chemical substances that can alter or affect the structure or function of the body.
They can be used for medicinal purposes or recreational purposes, as well as be addictive or non-addictive.
They can be classified as stimulants, depressants, opioids, hallucinogens, cannabinoids, and inhalants.
Why are Certain Drugs Addictive?
Drugs interfere with the ways that neurons interact with neurotransmitters. Some drugs, like marijuana, mimic the neurotransmitters in the brain, which allows them to activate certain neurons.
Marijuana is a type of cannabinoid, which is a class of chemical compounds from the cannabis plant that originated in Asia. The cannabis plant was first used to make ropes and textiles, but was later used for medicinal and spiritual purposes. Additionally, they can be medicinal, psychoactive, or non-psychoactive and stay in the body for 3-4 days after use.
THC, which is the main active component in marijuana, binds to the cannabinoid receptors in the brain. This binding mimics neurotransmitters and triggers a release of dopamine, and increased use of marijuana leads to more dopamine being released, creating a reinforcement loop that leads to addiction.
Medical marijuana / Harvard Health Publishing / Harvard Medical School
Although the chemicals in the drugs mimic the neurotransmitters, they are not exactly the same. This causes them to send abnormal messages and, in the case of some drugs like heroin, send an increase of dopamine because they bind to and activate opioid receptors. This also blocks the transmission of pain and causes a large amount of pain relief. Additionally, it can lead to dependence because it causes the brain to reduce the number of endorphins and the sensitivity of opioid receptors. Over time, the brain and body become dependent on external stimulants like heroin to feel any sense of happiness.
Heroin, another narcotic, is a very strong, highly addictive drug that comes from morphine, which is extracted from a part of the opium plant. It can cause severe withdrawal symptoms, overdose, liver and kidney disease, and many other negative side effects. Heroin can come in the form of a white or brownish powder, or a black, sticky substance. It is typically injected, snorted, or smoked and considered a Schedule I controlled substance in the U.S. and most other countries. That means that the drug is illegal, has a high potential for abuse, and is not accepted for any type of medical use.
Cocaine, another popular narcotic, comes from the leaves of a coca plant, native to South America, most commonly, Colombia, Peru, and Bolivia. Traditionally, people in the Andes chewed or brewed coca leaves as a medicine and stimulant; however, industrial processing has made their effects more potent, creating a drug trade. Cocaine is highly addictive and can cause serious health concerns like depression, bleeding in the lungs, and inflammation. Cocaine is illegal in the US, as it hijacks the brain’s reward system, causing a flood of dopamine and other neurotransmitters, but it can be used for medical purposes with restrictions. Over time, the brain and body become dependent on cocaine to feel any sense of happiness.
New Ingredient in Cocaine Vaccine Shows Promise in Mouse Study / Duke Health
These drugs affect the ganglia, a part of the brain responsible for relaying pleasurable effects and forming routines. The over-stimulation of a nerve cluster can lead to a feeling of euphoria or a dopamine release. The large amounts of dopamine make the brain connect drugs to the good feeling and teach the brain to continue using drugs. However, the ganglia are also the reason the drug’s high fades over time, as they adapt to its constant presence and become less sensitive to its effects.
Drugs are more addictive than natural activities that release dopamine, like working out, because drug misuse can lead to fewer neurotransmitters being released in general. This makes a person’s overall ability to feel pleasure for regular activities lower, making them feel flat or unmotivated in general. This also leads to people needing more and more drugs to feel a normal level of reward.
While many drugs are plant-derived and addictive, the rise of synthetic drugs is creating an unprecedented danger due to unnatural chemicals increasing the potency and unpredictability of the drug.
QUICK CAUTIONS: Synthetic Drugs
They are often illegal and have very little quality control, which makes the potency and effects of the drug unpredictable.
Synthetic drugs are easily contaminated with other hazardous materials, poisons, or drugs. Untested stimulants and chemicals may also exist in the drug, where the long-term side effects are unknown. For example, many drugs are often laced with the synthetic drug fentanyl, which is very strong and can increase the high, causing consumers to keep buying the drug. However, fentanyl is extremely deadly and a little amount can be fatal, leading to an increase in overdose deaths.
Manufacturers constantly modify the chemical structure of the drugs to increase the high and addictiveness of the drug as well as evade authorities. This also makes it harder for medical professionals to treat overdoses or reactions because they are not familiar with the drug.
Synthetic drugs are often sold under misleading names with colorful packaging to evade authorities, which can lead to accidental consumption. For example, Spice and K2 are common names for a lab-made drug that mimics the THC in marijuana by mimicking marijuana’s chemical structure. It is often sold under the name of herbal incense or potpourri to sound more enticing and evade authorities.
Synthetic drugs: Don’t ‘spice’ it up / Joint Base Langley-Eustis
How Scientists are Using Worms to Learn About Humans
Worms and humans could not possibly be any more different. And yet, scientists have been studying C. elegans (caenorhabditis elegans) to learn more about the human body over 70 years. These unassuming worms have aided in groundbreaking findings in medicine for human diseases such as Alzheimer’s, AIDS, and stroke.
What makes C. elegans so valuable is not its complexity, but rather its simplicity. Because so many of its biological pathways are conserved in humans, this worm provides a uniquewindow into the fundamental processes of life, including cell division, gene regulation, neural signaling, and aging. With a transparent body, rapid life cycle, and a genetic makeup that mirrors much of our own, C. elegans has become an essential organism in modern biomedical research. Understanding how scientists use these worms can help us appreciate not just what we’ve already learned, but also the vast potential that still lies ahead.
What is C. elegans?
C. elegans is a free-living nematode that has become one of the most important model organisms in research. It measures approximately one millimeter in length and naturally lives in temperate soil environments, where it feeds on bacteria like e. coli. It is non-parasitic and exists in two sexes: hermaphrodites, which are capable of self-reproduction, and males, which occur at a less than 0.1% chance under normal conditions. The hermaphroditic reproductive mode allows for the maintenance of isogenic populations, which is advantageous for genetic studies.
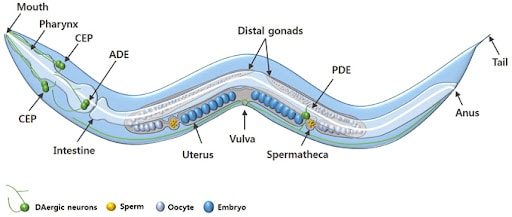
The adult C. elegans hermaphrodite has exactly 959 somatic cells while the adult male C. elegans has exactly 1,031 somatic cells. The worm’s relatively simple anatomy includes muscles, a nervous system, a digestive system, a reproductive system, and an excretory system. The organism develops through four larval stages before reaching adulthood, with a complete lifecycle taking just two to three weeks under laboratory conditions.
Genetically, C. elegans has a compact genome consisting of about 100 million base pairs across six chromosomes. It was the first multicellular organism to have its entire genome sequenced in 1998 in a project led by John Sulston and Bob Waterstons. Its genome is highly amenable to manipulation using a variety of modern techniques.
Why do scientists study C. elegans specifically?
First introduced into studies by Sydney Brenner in the 1960s to study neurological development and the nervous system, the nematode proved itself in the lab with its unique combination of genetic, anatomical, and practical features that make it exceptionally suitable for biomedical research.
Remarkably, around 60-70% of human disease-associated genes have counterparts in the C. elegans genome, making it an incredibly valuable model for studying human biology. Many genes responsible for critical cellular functions are evolutionarily conserved between worms and humans. Therefore, scientists can manipulate the function of these genes in C. elegans to study their roles in disease without the complexity or ethical challenges of working with human subjects or higher animals like mice or primates.
Adult hermaphrodites’ cells, which remain the same in every single worm, each of which has been identified and mapped, allowing for detailed tracking of development, differentiation, and cellular processes. Its transparent body enables real-time visualization of internal structures, including neurons, muscles, reproductive organs, and digestive tissues. The worm, which has a simple nervous system of only 302 cells, is one of the only organisms where every neural connection is known. Additionally, C. elegans has a short life cycle of two to three weeks and is easy to culture in large numbers, making it especially convenient for developmental and aging studies.
How do scientists modify C. elegans in experiments?
Scientists modify and study C. elegans using four primary methods: RNA interference (RNAi), CRISPR-Cas9 genome editing, transgenic techniques, and drug screening.
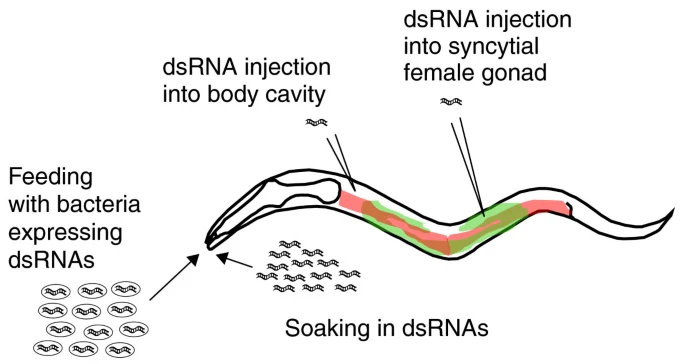
One of the most widely used techniques for modifying gene expression in C. elegans is RNA interference (RNAi). This method allows scientists to silence specific genes to observe the effects of their absence. In C. elegans RNAi can be easily administered by feeding worms with genetically engineered E. coli bacteria that produce double-stranded RNA (dsRNA) matching the gene of interest. Once ingested, the dsRNA activates the worm’s endogenous RNAi pathway, leading to the degradation of the corresponding messaging RNA and a reduction or elimination of the target protein. This method is highly efficient, non-invasive, and relatively easy to perform, making it ideal for large-scale genetic screens. Researchers can identify genes involved in key processes such as embryonic development, aging, metabolism, and neurodegeneration.
The CRISPR-Cas9 system has revolutionized genetic research in C. elegans by enabling precise, targeted alterations to the genome. Scientists introduce a complex composed of the Cas9 enzyme and a guide RNA (gRNA) into the worm, which directs the Cas9 to a specific DNA sequence. Once there, Cas9 introduces a double-strand break in the DNA. The cell’s natural repair mechanisms then fix the break, and researchers can insert, delete, or replace specific DNA sequences. In C. elegans, CRISPR can create mutants mimicking human disease alleles or study regulatory elements of genes. This method provides a level of control that surpasses RNAi, as it allows for permanent and heritable genetic modifications. Scientists often inject the CRISPR-Cas9 components directly into the gonads of adult hermaphrodites, ensuring that the genetic changes are passed onto the offspring.
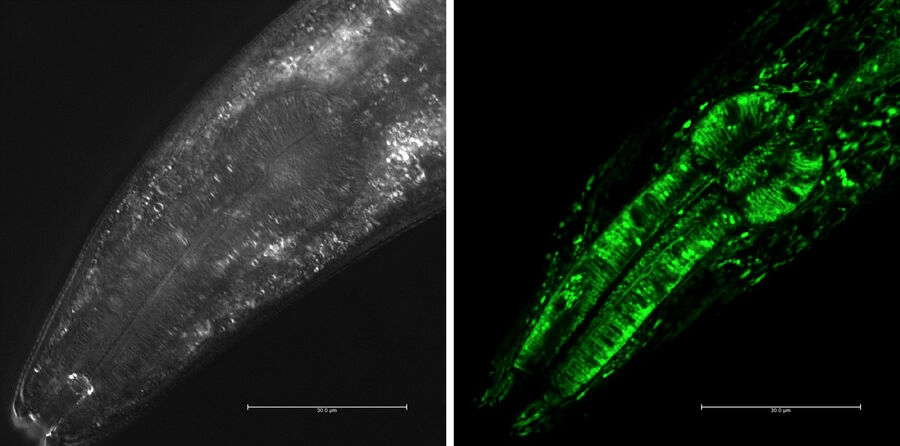
Transgenic techniques in C. elegans insert foreign DNA into the worm’s genome to monitor gene expression, trace cell lineages, or study protein localization. One common approach is to fuse a gene of interest to a reporter gene such as green fluorescent protein (GFP). When this gene is expressed, the fluorescent tag can be visualized in living worms using fluorescence microscopy. This allows researchers to observe where and when specific genes are active, how proteins move within the cells, and how cells interact during development or disease progression. Transgenes are typically introduced via microinjection into the syncytial gonads of adult worms, leading to the formation of extrachromosomal arrays inherited by the next generation. Stable lines can also be created through CRISPR or chemical integration methods. These visual tools are particularly powerful due to the worm’s transparent body, which makes it possible to track fluorescent signals in real time throughout the entire organism.
C. elegans is an excellent system for drug screening and environmental toxicology due to its small size, short lifespan, and genetic tractability. Researchers can test the effects of thousands of compounds quickly and cost-effectively. In these experiments, worms are exposed to chemical agents in liquid or on agar plates, and their survival, movement, reproduction, or specific cellular markers are measured to assess the biological impact. Using genetically modified strains that mimic human disease pathways, scientists can screen for drugs that alleviate symptoms or restore normal function. These tests provide an efficient first step in drug development, singling out promising candidates before moving onto mammalian models.
The cell lineage and the programmed cell death in C. elegans / Nobel Prize in Physiology or Medicine 2002
One of the most groundbreaking discoveries made using C. elegans was the genetic basis of programmed cell death, or apoptosis, a critical process in both development and disease. The research was led by Dr. H. Robert Horvitz at the Massachusetts Institute of Technology. Horvitz and his colleagues began studying cell death in C. elegans in the 1980s by tracing the fate of every cell in the worm’s body during development. They discovered that exactly 131 cells always die in the developing hermaphrodite and that this process was genetically controlled. Through genetic screening, Horvitz identified three core genes that regulated apoptosis: ced-3, ced-4, and ced-9. By inducing mutations in these genes, the researchers could either prevent or accelerate cell death in the worm. This revealed that cell death is not a passive consequence of damage, but rather an active, genetically programmed event. The mammalian counterparts of these genes, like caspases and BCL-2, were later discovered to play central roles in cancer, autoimmune diseases, and neurodegeneration, making this research foundational to modern medicine. Horvitz was awarded the 2002 Nobel Prize in Physiology or Medicine for his work along with Sydney Brenner and John Sulston.
In addition, C. elegans has contributed to our understanding of neurodegenerative diseases such as Alzheimer’s. One major study was led by Dr. Christopher Link at the University of Colorado in the late 1990s. Link developed a transgenic C. elegans strain that expressed the human β-amyloid (Aβ) peptide in muscle cells. This is the same peptide that forms toxic plaques in the brains of Alzheimer’s patients. In the study, the researchers observed that worms expressing Aβ developed progressive paralysis as they aged, mimicking aspects of human Alzheimer’s pathology. They then used this model to screen for genetic mutations and chemical compounds that could suppress the toxic effects of Aβ. Their work identified several genes involved in protein folding and stress response that modified Aβ toxicity. This demonstrated that C. elegans could be used as a fast and cost-effective in vivo system for identifying genetic and pharmacological modifiers of Alzheimer’s disease. The worm model has since then been adapted by numerous labs worldwide to study tau protein aggregation and mitochondrial dysfunction, expanding our knowledge of neurodegenerative pathways.
Another major discovery made using C. elegans was the link between insulin signaling and lifespan regulation. Dr. Cynthia Kenyon at the University of California, San Francisco, led a series of experiments in the 1990s that transformed the field of aging research. Kenyon’s team discovered that a single mutation in the daf-2 gene, which encodes an insulin/IGF-1 receptor, could double the worm’s lifespan. They found that when daf-2 signaling was reduced, it activated another gene, daf-16, which promoted the expression of stress-resistance and longevity-related genes. To test this, Kenyon used genetic mutants and tracked their development and survival across generations. The C. elegans with the daf-2 mutation lived significantly longer than their wild-type counterparts and were more resistant to oxidative stress and heat. These findings provided the first clear evidence that aging could be actively regulated by specific genetic pathways rather than being a passive deterioration process. Later studies found that similar insulin/IGF-1 pathways exist in mammals, including humans, opening new therapeutic avenues for age-related diseases, diabetes, and metabolic disorders.
So what does the future hold?
The future of C. elegans in scientific research is remarkably promising, with its applications continually expanding as technology and genetic tools advance. With the rise of CRISPR-Cas9, optogenetics, and high-throughout screening techniques, researchers can now manipulate C. elegans with unprecedented precision to study complex biological processes such as epigenetics, gut-brain interactions, and real-time neuronal activity. In the coming years, C. elegans is expected to play an even greater role in personalized medicine and systems biology. Its potential as a predictive model for human gene function could aid in understanding the consequences of mutations found in patient genomes, leading to more tailored treatments. The worm’s short life cycle, fully mapped genome, and conserved biological pathways make it an ideal model for rapidly identifying new therapeutic targets and testing drugs, especially for age-related and neurodegenerative diseases. Despite its simplicity, this tiny nematode continues to open doors to complex human biology, proving that even the smallest organisms can have the biggest impact on science and medicine.
“C. Elegans 101: A White Paper – InVivo Biosystems.” InVivo Biosystems, 26 Jan. 2024, invivobiosystems.com/disease-modeling/c-elegans-101-a-white-paper/.
Edgley, Mark. “What Is Caenorhabditis Elegans and Why Work on It? – Caenorhabditis Genetics Center (CGC) – College of Biological Sciences.” Umn.edu, University of Minnesota, 2022, cgc.umn.edu/what-is-c-elegans.
Venkatesan, Arun, and Krishma Adatia. “Anti-NMDA-Receptor Encephalitis: From Bench to Clinic.” ACS Chemical Neuroscience, vol. 8, no. 12, 7 Nov. 2017, pp. 2586–2595, https://doi.org/10.1021/acschemneuro.7b00319.
Wheelan, Sarah J, et al. “Human and Nematode Orthologs — Lessons from the Analysis of 1800 Human Genes and the Proteome of Caenorhabditis Elegans.” Gene, vol. 238, no. 1, Sept. 1999, pp. 163–170, https://doi.org/10.1016/s0378-1119(99)00298-x.
“Whitehead Institute of MIT.” Whitehead Institute of MIT, wi.mit.edu/unusual-labmates-how-c-elegans-wormed-its-way-science-stardom.
“Wonderous Worms.” NIH News in Health, 3 July 2025, newsinhealth.nih.gov/2025/07/wonderous-worms. Accessed 1 Aug. 2025.
Zhang, Siwen, et al. “Caenorhabditis Elegans as a Useful Model for Studying Aging Mutations.” Frontiers in Endocrinology, vol. 11, 5 Oct. 2020, https://doi.org/10.3389/fendo.2020.554994.
Have you ever had a parasite? Maybe you ate an unwashed fruit, had an open wound, or even stepped on something you shouldn’t have. Nevertheless, parasites are everywhere and more common than you may think. In this article, we’ll go over parasites as a whole; including a review on what they are, theories on evolution, and a deep dive into a specific parasite. Overall, parasitism is one of the most complicated relationships seen in nature, and whilst it’d take a mountain of explanation to understand it all, hopefully this article can deepen your current understanding and offer some insightful information.
What Are Parasites?
By definition, parasites are organisms that live off of another organism or “host”. There are many “species” or categories of parasites, ranging from utterly harmless to ultimately fatal. Some of the more common parasites you may have heard of include tapeworm, roundworm, pinworm, etc. While there are countless ways to get infected, tapeworm for example, only needs its eggs to be accidentally swallowed . Fortunately such cases are rare in developed countries like the U.S. Additionally, these parasites are objectively easy to get rid of. Albendazole is a very common medication used to treat parasitic worm infections, and taking a few doses should cure the disease. Oftentimes, albendazole is crucial in mass drug administration as an attempt to control and lessen cases of infection, especially within developing countries.
So what happens when you get a parasite? Well, it is impossible to give one direct answer. Say you are infected with a common intestinal worm, perhaps unknowingly you have ingested pinworm eggs. Some symptoms might include gastrointestinal issues, vomiting, abdominal pain, extreme itching, and even irritation, all common with other intestinal parasites. You go to the doctor, get some blood work, and thankfully they diagnose you, treat you with albendazole, and everything is back to normal. But what about when it’s not that simple?
Some parasites are much more dangerous, and at times, even incurable. Malaria, a very widely known global health concern, is a single-celled parasite spread by mosquitos. In some cases, such as that of Plasmodium falciparum (the most dangerous type of malaria) once infected, it can take only 24 hours to kill. While there are treatments and improvements in the medical world for malaria, developing countries are still struggling with the disease to this day. Another deadly parasite is brain-eating amoeba or Naegleria Fowleri. Found in infected waters such as lakes, this parasite enters the brain through the nose while you are swimming. While it is extremely rare, fatality rates are nearly 100 percent. Naegleria fowleri destroys the brain tissue causing swelling and oftentimes complete coma. Once the symptoms set in within a week of infection, it will take roughly five days until death. Unfortunately, there are countless more of these dangerous parasites including schistosomes, which we will cover later. However for now, let’s see how these parasites came to be.
The Evolution of Parasites
Though there are countless theories determining the exact evolutionary path or origin of parasites, there is no factually known truth. Overall, the study of evolution of organisms is an extremely difficult and unending task. To truly form a complete cycle of evolution you have to not only know the events that took place, but their total effect and order., Unfortunately we cannot go back into the past, but, there are some pretty strong theories regarding parasite evolution.
It is safe to presume that parasites arose millions of years ago from previously freeliving organisms. Many researchers believe that the majority of present-day parasitic life forms evolved after being ingested by their host. This theory, called ‘freeliving ancestors’, describes how freeliving organisms evolved to survive within their host by gaining their needed nutrients from within the host’s stomach. As mentioned earlier, some of the most common or well known parasites, such as the tapeworm, show stark similarities with this theory.
On the other hand, another well known potential theory is that the parasite-host relationship may have formed from a predator-prey relationship, where the parasite acts as the predator. Ancestors of such parasites have been found to have collected similar nutrients from their prey as parasites collect from their host. This theory is common in ectoparasitism, in which the parasite lives within, or on, the host’s skin.
Another theory to consider are facultative parasites. This represents the “hybrid” of parasitic characteristics and regular freeliving organisms. They provide the possible transitional state, or the “evolutionary stepping stones” within the transition to full blown parasitism. Facultative parasites can survive both on their own, and within, or on, a host. While dissecting facultative parasites as a whole calls for a separate discussion, it is important to understand a few things, for one: phenotypic plasticity. This refers to the flexibility of an organism’s phenotype, or observable characteristics. An organism with strong phenotypic plasticity has the ability to adapt more fluidly to its environment. For example, a facultative parasite may increase survival under specific conditions and overtime adapt on favorable heritable variations (in this case: parasites), also known as the Baldwin effect. Similar to the Baldwin effect, genetic assimilation, which represents phenotypic plasticity under specific conditions as well, is more set in place. This implies that eventually the organism’s plasticity will decrease, and the trait will no longer need the environmental trigger for it to show as it becomes fixed or stuck in place.
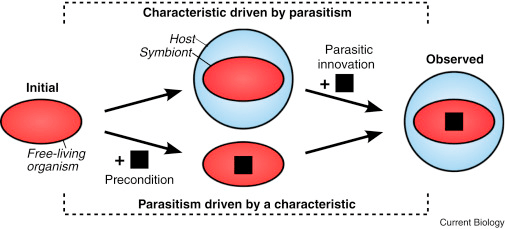
Once again, even with immense research and evidence, the exact path of evolution for parasites is difficult to place. Even with potentially knowing events that were detrimental to the evolutionary path, we still cannot specifically know which traits may have caused what. An interesting metaphor would be to think about how “noses might not have been selected to carry glasses.” While the characteristic of having a nose is useful for wearing glasses, it certainly didn’t evolve for that reason. Likewise, just because an organism has a quality that relates to parasitism, it may have nothing to do with it. For example, some traits we may have thought were specific to the evolution of parasites, have been found in completely different freeliving organisms with no real connection. Additionally, a parasitic trait can evolve in different ways as well. For example, the image below demonstrates the inverse relationship between various characteristics and parasitism.
There are many misconceptions when it comes to parasites. Admittedly, parasites are utterly terrifying, so intense phobias and even psychosis aren’t farfetched. However, these false beliefs can lead to incorrect, useless, and even sometimes harmful homemade “treatments”. For example, have you ever heard of a parasite cleanse? A parasite cleanse is a form of detoxing the body through supplements, diets, or drinks. They frequently include different types of herbs, oils, and other supplements. These “treatments” are not medically necessary nor are they FDA approved. There is no evidence of these cleanses treating any parasites, and sometimes they can be harmful to your gut, causing other issues. If you believe you may be infected with a parasite, it is important to get proper medical help. That being said, let’s look into the current state of the medical world in relation to parasites.
According to the World Health Organization, or WHO, approximately one quarter of the world’s population is infected with some type of intestinal worm, with even higher rates in developing countries. Although this statistic might seem concerning, there have been many improvements in the medical world, as well as constant research being done. For one, the mass drug administration system, as mentioned once earlier, is seeing vast improvements with providing ample medicine and treatments to those who need it. In particular, nanotechnology, the method of manipulating matter at the near-atomic scale, has helped tremendously in targeted drug delivery. Deeper research regarding genes and interactions of parasites with the host, is assisting in the making of treatments and vaccines. Whilst parasitic infections remain a problem today, there is much hope to help the issue decline within the future.
Schistosomes
By now you have read through much information about parasites, specifically what they are, their evolution, and even some medical overviews. So now let’s take a deep dive about a specific parasite: Schistosomes. Schistosomes are a type of parasitic flatworm, distinctively known as blood flukes, and are the root of a terrible, oftentimes chronic disease called schistosomiasis. So what do you need to know?
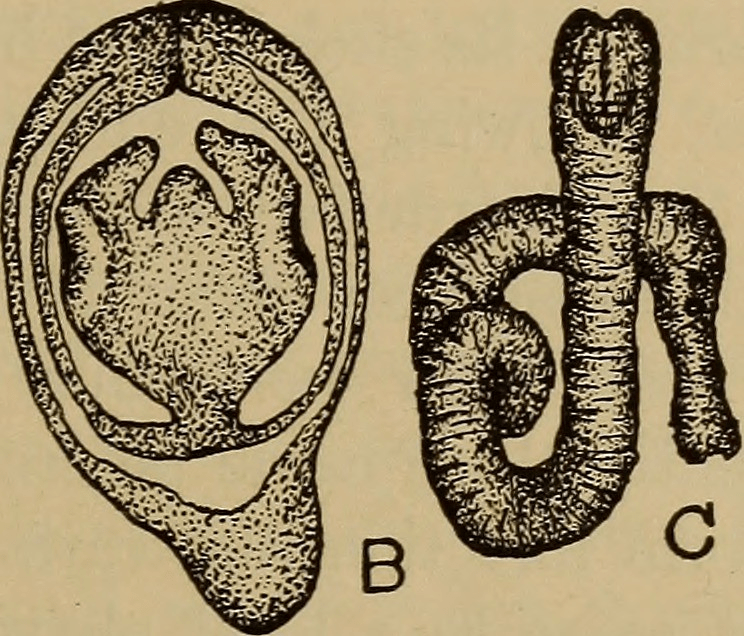
Schistosoma are believed to have originated in the supercontinent of Gondwana around 120 million years ago, from their early parasitic ancestors, which primarily infected hippos. Interestingly, they began their life by primarily infecting a snail, parallel to their life cycle today, which you’ll read about later. From that point, through host migration, they traveled to Asia and Africa, where they are primarily found today. Eventually, the parasite evolved into other forms, more specifically schistosoma, predominantly infecting humans.
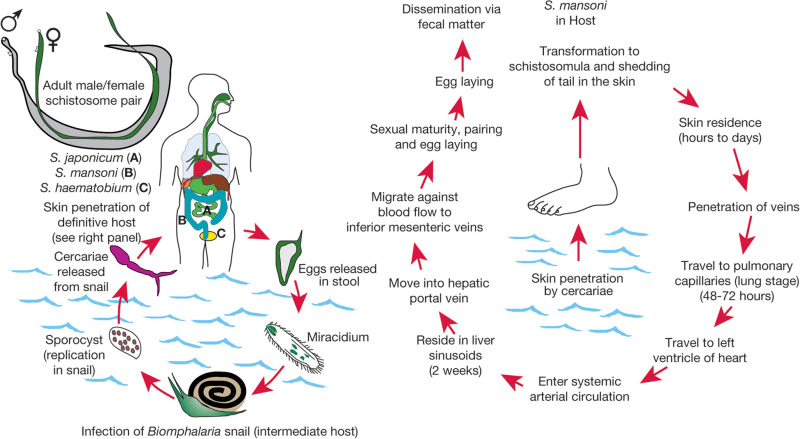
The life cycle of schistosoma has many stages, including two hosts. First, eggs are passed down from the previous host, through urine or stool, into water. These eggs, which then hatch into larvae, must now find their first host: a snail. Within these snails, the schistosoma continues to mature, releasing once again into water. As you are harmlessly swimming or bathing in seemingly clean waters, the schistosoma penetrates the skin, entering and infecting your body. From that point, they travel to your liver, where they fully mature into adult worms, and travel to the veins in the intestines or bladder to mate soon after. At this point you could have been infected for potentially months. Other than a slight skin irritation where they had entered your body previously, you don’t start showing symptoms until you get Katayama fever or the acute stage of schistosomiasis, lasting for a couple weeks.
Katayama fever is a hypersensitivity or immune complex reaction to the eggs being deposited in the body’s tissue. Symptoms of this stage are categorized by fever, abdominal pain, cough, muscle and joint pain, and so much more. At this point the disease is still possibly reversible. Treatments such as preziquantel are common for treating this disease and can help those infected formulate a full recovery. However, some people don’t necessarily show symptoms until it’s too late. For instance, in 2021 an estimated 176.1 million out of 251.4 million people were not treated on time.
The next stage is chronic Schistosomiasis. While technically the worms can be killed through specific treatment, they can cause irreversible organ damage with life long affects. Furthermore, the long lifespan of the adult worms can make it exceedingly difficult to treat. These worms can live in the body for over a decade, laying hundreds of eggs daily. While these eggs are produced in order to be released in the urine and stool, they frequently get trapped in the tissues of your organs. As they get trapped, the body’s immune response causes extreme inflammation in the organs, primarily the liver, bladder, and intestines. Alongside many other implications due to the lodging of the eggs, such as fibrosis (the formation of scar tissue), can lead to organ failure, increased risk of cancer, and ultimately death.
Those with schistosomiasis often spend their lives in and out of hospitals. As time goes on, their bodies begin shutting down or falling victim to other illnesses. Schistosomiasis is an extremely hard disease to deal with, infecting more than 200 million people worldwide. Developing countries in Africa and Asia struggle tremendously, especially without access to clean water, or the inability to receive necessary treatment.
Though the probability of completely eradicating the disease within the near future is low, thankfully the number of infected is generally decreasing. As immense efforts are being made globally, better access to medication, as well as sanitary environments are readily being provided. Additionally, extensive amounts of research are helping find out more about schistosoma to better our treatments and potentially develop a vaccine.
Conclusions
Overall, while parasitic infections are fortunately majority of the time treatable, there is so much more to them than what one might think. In this article we were able to cover plentiful information about parasites, their evolutionary history, and the terrifying reality of Schistosomiasis, so with this knowledge, it is time to make a real impact. Below, there is a link to a GoFundMe page, where you can help Recy Abellanosa, a mother, wife, and teacher who is struggling with the effects of schistosomiasis. By donating, you will be able to take some of the financial burden off her family as she fights the disease. As a final remark, I highly encourage you to learn more about these organisms, as well as keep yourself and others around you educated in the current scientific and medical world.
Baker, J. R. (1994). The origins of parasitism in the protists. International Journal for Parasitology, 24(8), 1131–1137. https://doi.org/10.1016/0020-7519(94)90187-2Luong, L. T., & Mathot, K. J. (2019). Facultative parasites as evolutionary stepping-stones towards parasitic lifestyles. Biology Letters, 15(4), 20190058. https://doi.org/10.1098/rsbl.2019.0058
Gobbi, F., Tamarozzi, F., Buonfrate, D., van Lieshout, L., Bisoffi, Z., & Bottieau, E. (2020). New Insights on Acute and Chronic Schistosomiasis: Do We Need a Redefinition? Trends in Parasitology, 36(8), 660–667. https://doi.org/10.1016/j.pt.2020.05.009
Janouskovec, J., & Keeling, P. J. (2016). Evolution: Causality and the Origin of Parasitism. Current Biology, 26(4), R174–R177. https://doi.org/10.1016/j.cub.2015.12.057
Pion, S. D. S., Chesnais, C. B., Bopda, J., Louya, F., Fischer, P. U., Majewski, A. C., Weil, G. J., Boussinesq, M., & Missamou, F. (2015). The impact of two semiannual treatments with albendazole alone on lymphatic filariasis and soil-transmitted helminth infections: a community-based study in the Republic of Congo. The American Journal of Tropical Medicine and Hygiene, 92(5), 959–966. https://doi.org/10.4269/ajtmh.14-0661
Tiwari, R., Gupta, R. P., Singh, V. K., Kumar, A., None Rajneesh, Prasoon Madhukar, Sundar, S., Gautam, V., & Kumar, R. (2023). Nanotechnology-Based Strategies in Parasitic Disease Management: From Prevention to Diagnosis and Treatment. ACS Omega, 8(45), 42014–42027. https://doi.org/10.1021/acsomega.3c04587
Huntington’s Disease, discovered by George Huntington in 1872, is a hereditary genetic brain disorder. Since then, many researchers have dedicated their lives to studying Huntington’s Disease. While we have not found a cure nor treatments to slow the progression, we have discovered how it works, what it is, what it can do, and how it is passed down.
George Huntington, an American physician from Long Island with a degree from Columbia University, published his paper “On Chorea” in 1872, describing Huntington’s Disease so accurately and succinctly that the disease was named after him. He was only 21 when his paper was published. However, he first encountered what would come to be known as Huntington’s Disease when he was 8 years old while accompanying his father and grandfather on medical rounds. Within “On Chorea”, he summarized three key characteristics of a person with Huntington’s Disease: their propensity to suicide and mental disorders, inheritance patterns, and progressive disabilities. This was his sole contribution to medical research. His paper shone a light on this “medical curiosity” from a new field of medicine and shook the medical research world into a frenzy to try to grasp what Huntington’s was and how it worked.
Huntington’s Disease (HD), is inherited from your parents following an autosomal dominant inheritance pattern. It causes nerve cells, mainly in the basal ganglia, brain cortex, and the striatum, to gradually break down and lose function. More than 15,000 Americans currently have HD, but many more are at risk of developing it. There are two kinds of Huntington’s Disease, adult onset, the most common, and early onset, which affects children and teenagers. Fortunately, early onset is very rare, only affecting 5.7% of Huntington’s cases. HD affects an estimated 3 to 7 people out of 100,000, most commonly people of European descent. If a parent has HD, their child has a 50% chance of inheriting the genetic mutation as well. If the child does not inherit it, they will not show symptoms and cannot pass it down. On the condition that the patient has more than 50 CAG repeats, there is a 90% chance they inherited the gene from their father, because CAG repeats tend to be more unstable when passed from the male. There are situations where HD occurs without family history. This event is called Sporadic HD.
Huntington’s is a genetic mutation of the HTT gene. It produces a protein called huntingtin. This protein helps your nerves function. The HTT gene is found on chromosome 4, which also happens to be associated with the cause of many other genetic disorders and some types of cancer. The defect involves a DNA segment known as CAG trinucleotide repeat. It is made up of three DNA building blocks, cytosine, adenine, and guanine, appearing several times in a row. Normally, the CAG segments are repeated 10 to 35 times within a gene, and these people lie in the unaffected range, whether normal or intermediate allele sub-ranges. To a person with Huntington’s, it can be repeated 36 to more than 120 times. They lie in the affected range, either reduced penetrance or full penetrance if they have more than 40 CAG repeats. People in the intermediate allele and the reduced penetrance sub-ranges, with 27-39 CAG repeats, may not develop symptoms but can be carriers. The increase in repeats leads to the production of abnormally long and oddly shaped huntingtin proteins. The elongated protein forms toxic fragments that fuse together and collect in neurons, disrupting the normal function of cells and ultimately killing them. This causes the symptoms of Huntington’s Disease. As the mutated HTT gene is passed down, the amount of CAG trinucleotide repeats increases. A larger number of repeats causes early onset Huntington’s and a sooner appearance of symptoms. This is referred to as anticipation.
The diverse symptoms of Huntington’s Disease are what leads to many misdiagnoses in the early stages and why it took so long to be recognized as its own disease. George Huntington’s paper “On Chorea” focused mostly on chorea, which involves involuntary jerking or writhing movements, akinesiadeveloping as the disease progresses, unusual or slow eye movements, trouble with walking and balance, dystonia, ataxia, trouble with speech, athetosis, and dysphagia, and weight loss. Mental health conditions include irritability, mood swings, social withdrawal, insomnia, fatigue, loss of energy, suicidal thoughts, OCD, mania, bipolar disorder, psychosis, hallucinations, and paranoia. There are cognitive conditions as well, like, trouble organizing, trouble prioritizing and focusing on tasks, lack of flexibility and perseveration, lack of impulse control that can lead to violent outbursts, lack of awareness in one selves behaviors and ability, slowness in processing thoughts, seizures, trouble with driving, and trouble learning new information and memorization. These symptoms can get more intense when the person is nervous or distracted. Eventually, these symptoms get so bad that it is more closely categorized as dementia.
Many people with HD remain conscious of their environment and can express emotions. As it progresses, the patient will need more help and supervision. Ultimately, they will need help at all hours of the day. HD is not fatal in and of itself. Patients most commonly die from complications like physical injury from falls and accidents, malnutrition due to trouble feeding oneself, infections, typically pneumonia but others as well, choking, heart failure, seizures, and, due to the mental toll, 7-10% of HD patients commit suicide. The average lifespan of a person with Huntington’s is 10 to 30 years after a diagnosis.
This disease, because of its diverse symptoms, takes a skilled eye to diagnose. In most cases, it can be done with a neurological exam and an analysis of the patient’s medical and family history. But in other cases, the patient might require genetic and blood tests and diagnostic imaging like an MRI, CT, PET scan, or EEG. A neurologist and neuropsychiatrist will perform these tests. There are many research studies underway to study Huntington’s and while we do not have a cure, we have a basic understanding of the disease, which means we are one step closer to long term treatments. Johns Hopkins, for example, has 4 ongoing studies: the Sage Studies: PERSPECTIVE Program, which is evaluating the safety and efficiency of the experimental drug SAGE-718 in adults with early Huntington’s Disease, the Generation HD2 tests, which is the second phase of tests on Tominersen in young adults with HD ranging from 25-50 years old. The HDClarity study, an observational study to collect cerebrospinal fluid in order to study biomarkers that influence HD’s pathophysiology and growth, and the Enroll-HD program, a registry for the Global Huntington Disease Cohort, providing vast information for future clinical research. These are just a few of the many programs dedicated to unlocking the mysteries of HD. The most promising fields are those studying biomarkers, like the HDClarity study, and stem cell research.
There are many options for treatments that can help improve the quality of life for a person with HD. They will require more help as the disease progresses and a team of people to help them like a neurologist, psychiatrist, genetic counselor, physical therapist, occupational therapist, and a speech therapist. A counselor could also help the patient and their family members with the emotional toll. Medications can also be prescribed to ease symptoms and keep them functioning as long as possible. To treat chorea they could take deutetrabenazine, amantadine, tetrabenazine, or haloperidol. The latter two of which could also help deter hallucinations and delusions. To manage their emotions, they could be prescribed antidepressants like fluoxetine and sertraline, antipsychotic drugs like risperidone and olanzapine; however, some antipsychotic medications have side effects that could make chorea and akinesia worse, and mood stabilizing medications like lithium. Antidepressant and antianxiety medications are also commonly prescribed because there are high rates of depression and suicide amongst patients with HD. It is also recommended to maintain physical fitness because it is shown that patients who exercise regularly delay the symptoms of HD more than those who do not. Huntington’s, however, can be prevented by genetic counseling, prenatal testing, and in vitro fertilization, where an egg and sperm are fertilized in a lab and checked to see if it has Huntington’s disease. If it does not, it is then implanted back into the uterus. It is important to speak to a genetic counselor before having a child if you or your partner has HD or is at risk to develop symptoms.
An HD diagnosis is certainly not a death sentence. A person with Huntington’s can live a long, happy life. We now know so much about this disease that even George Huntington would not be able to believe. There are many options for every particular patient and every particular case. And as science and technology advances, so will we in our path to finding a cure for Huntington’s Disease.
Glossary
1. A CAG trinucleotide repeat is an unstable expansion of the DNA sequence “cytosine-adenine-guanine” (CAG) that codes for the amino acid glutamine, resulting in a long “polyglutamine” tract within a protein
2. a situation where individuals who inherit a disease-causing genetic mutation do not develop the associated disease or condition
3. Akinesia: become rigid (stiff) and move very little or not at all
4. Dystonia: unusual fixed (unchanging) postures
5. Ataxia: loss of coordination
6. Athetosis: slow, involuntary, and writhing movements
7. Dysphagia: difficulty swallowing
8. Psychosis: losing some contact with reality
9. Tominersen: a treatment for Huntington’s Disease that is under research and trials
Earlier this summer, I was graciously given the opportunity to shadow a private-practice oncologist/hematologist in the Dallas area. There, I gained a clear understanding of what a career in STEM entails, learned how doctors approach complex cancer cases, and secured an inside view into the emotionally taxing yet deeply rewarding work of an oncologist.
What does an Oncologist’s career look like?
At the ground level, an oncologist’s job involves diagnosing and treating cancer. They play a central role in administering cancer treatments and developing long-term plans. There are three main types of oncologists:
Medical Oncologist: Dr. Nair, whom I shadowed, practices as a medical oncologist. These doctors use targeted therapies like chemotherapy and immunotherapy to treat cancers.
Surgical Oncologist: Surgical oncologists perform biopsies and remove tumors through surgical procedures. Usually, after a medical oncologist has successfully shrunk a tumor through targeted therapy, a surgical oncologist will excavate the remaining piece.
Radiation Oncologist: As the name suggests, these doctors treat cancer through radiation therapy.
Dr. Nair works as a hematologist-oncologist. Because cancer often involves blood and bone marrow (leukemia, lymphoma, myeloma), having training in both oncology (solid tumors) and hematology (blood disorders) allows a doctor to treat a wider variety of patients without having to refer them to another clinic. Also, in the U.S., most oncologists need no extra schooling to end up board-certified in both.
Typically, becoming an oncologist requires about 14-16 years of school. This includes a four-year undergraduate program, where students generally major in biology, chemistry, mathematics, or physics. Then, students take the MCAT, or the Medical College Admission Test, and attend medical school to earn their MD. After four years of medical school, doctors attend a three-year residency program. Finally, they complete a three-year fellowship program, subspecializing in oncology or hematology-oncology. Oncologists typically finish schooling in their mid-thirties, and though they spend most of their twenties in schooling, many agree that this time is fully necessary due to the extensive information students have to understand.
A central part of an oncologist’s job is responding to a wide spectrum of questions, ranging from emotional ones like “if the tumor is getting bigger, do I have less time to live?” to straightforward questions like, “if I eat and sleep more, will I have more energy the next morning?” Sure, many of these questions become routine over time, but it’s that rare, complex one that truly tests a doctor’s knowledge and, when answered well, builds even more trust between the patient and their provider. Because cancer is such a serious topic, patients seek oncologists who make them comfortable, and the best way to provide that security is by easing their uncertainties and reinforcing confidence in their provider. This is exactly why those 14 long years of medical training matter so much.
The Difference Between Private Practice and Clinic
Dr. Nair is affiliated with the broader group Texas Oncology and practices at Medical City Dallas, but before going in to shadow her, I had no idea what the difference between a private practice and a clinic was. Here is an easy way to break it down:
Private practice: When a doctor or group of doctors owns, manages, and runs their own medical office. Like a business, they hire staff, manage billing, and run their own practice from top to bottom. Though private practice intersects the two contrasting fields of medicine and business, these doctors have more flexibility when not working for a large hospital or healthcare system.
Clinic: Usually affiliated with a larger group, hospital, or university. Doctors who work as part of a clinic follow the protocol set up by a broader employer and focus less on business and management.
Highlight Patients
You may think that looking at cancer gets repetitive after a while, and maybe you’re right- but in the two weeks that I shadowed Dr. Nair, we saw a wide variety of patients that kept me quite interested. Often, it wasn’t the cancer or condition that made them memorable, but their personality, and the reminder that cancer does not discriminate. People from all walks of life, rich or poor, tall or short, male or female, can be struck by the disease at random and affected in similar ways.
1. Female, mid-40s, obese
This patient was on blood-thinners that were administered by the hospital. Upon arriving home, she purposefully took double the prescribed dose for a few days. With the alarmingly high dosage this patient was taking, her gums would bleed when brushing her teeth, and minor cuts would bleed profusely without stopping. Suddenly, the patient formed a massive internal hemorrhage in her stomach, and was rushed to the ICU where she took a break from blood thinners and recuperated.
2. Female, mid-30s
This patient was aware she had a tumor in her lungs, but didn’t know the extent of its spread or whether it was even malignant. As the cardiothoracic surgeon opened her chest to perform a biopsy and assess the situation, he found that the cancer presented as stage 4 and had spread extensively throughout the lungs. After removing substantial diseased lung tissue, the patient’s remaining lung capacity was too low to sustain oxygenation. Therefore, she was placed on a ventilator that essentially acted as a pair of bedside lungs, pumping air for her.
3. Female, early-60s, groaning in pain
As Dr. Nair and I walked into the patient’s room, she was lying on the bed, groaning and screaming in severe pain. This woman had a pancreatic tumor, one of the most painful types of cancer, due to the tumor pressing on bunches of nerves and organs in the abdomen and back. Though she was fully lucid, the pain was preventing her from formulating complete thoughts or ideas, and her husband described that she could not eat properly or move around without a wheelchair. Dr. Nair told the couple to visit the ER within the hospital immediately, so that the patient could be administered stronger pain medications.
The role of women in healthcare
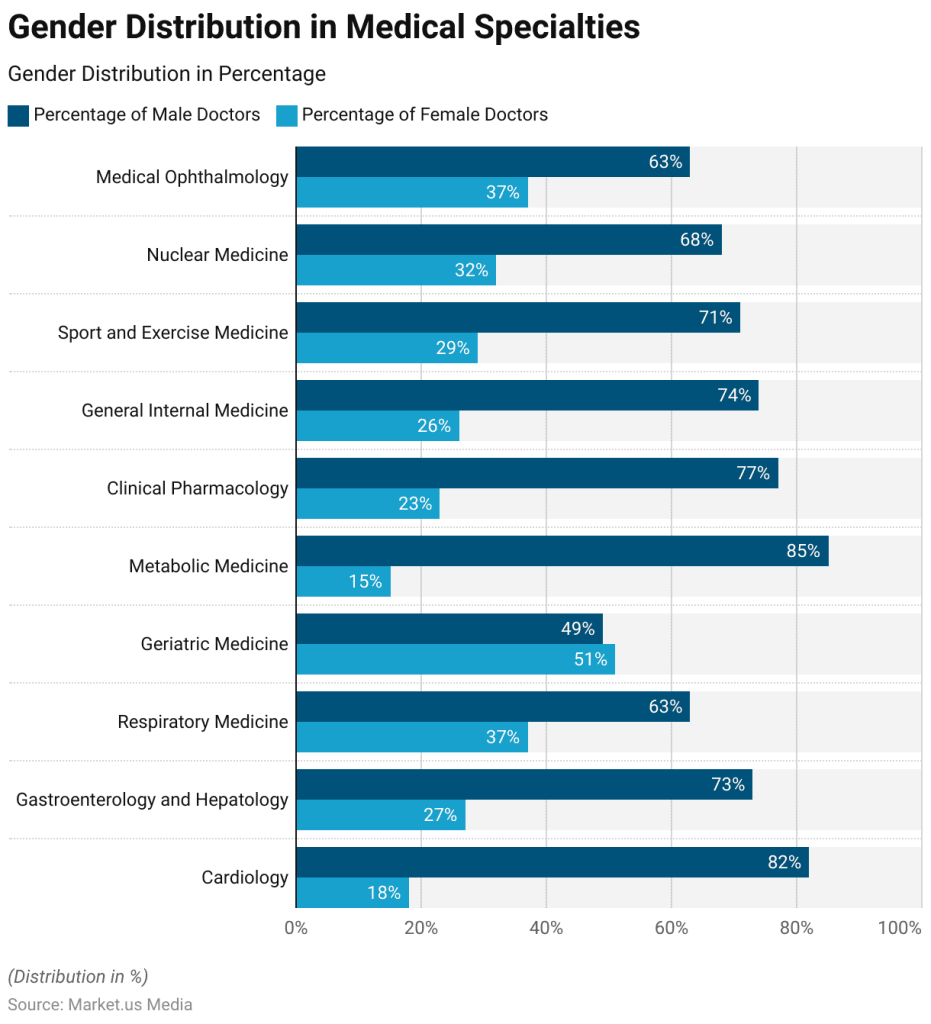
One thing that really stuck out to me was the number of women who worked in the office with Dr.Nair. Out of the three oncologists, only one was a man, and the rest of the staff, including the P.A. and infusion nurses, were all women.
In fact, according to the U.S. Bureau of Labor Statistics; around 77.6% of all healthcare workers are women. However, we hold a disproportionately small number of leadership positions compared to men. Where 77.6% of healthcare workers are women, only about 38% of all physicians are women.
Despite the gender gap that still exists today, equality growth in the last 20 years alone has been monumental. According to the Association of American Medical Colleges,
“From 2004 to 2022, the number of women in the active physician workforce increased 97%.”
Going forward, the future looks bright too. In 2019, women for the first time accounted for a majority (50.5%) of students enrolled in medical school in the United States. Today, women account for about 54.6% of medical school students. As women make up the majority of medical school graduates, the number of physicians in the coming years will consequently increase.
Conclusion
Before I arrived at the oncologist’s office, I pictured a gloomy waiting room filled with silent, dejected patients. Instead, I discovered something completely different. People tend to imagine only the sickest patients at a cancer clinic, the ones who are dying. But they often forget about the many who are improving, on the uphill climb, and who see the doctor’s office not as a place of punishment or despair, but as a lifeline that offers hope and light at the end of the tunnel.
Seeing this side of cancer care reshaped my view of healthcare entirely. It made me realize that medicine isn’t just about treating disease and sending patients on their way, but instead creating an environment where people are given a reason to keep fighting.
“Not only are plastics polluting our oceans and waterways and killing marine life – it’s in all of us and we can’t escape consuming plastics,” says Marco Lambertini, Director General of WWF International [20].
The emergence of plastic and its accumulation in people and the environment has been a rising global concern for over 80 years, since it first caught the attention of scientists in the 1960s due to the observed effects in marine species [7]. Even more concerning, plastics continue to accumulate on the planet year after year. In 2019, there were a predicted 22 million tons of plastic worldwide, with a projected 44 million tons of plastic polluting our earth within the next 35 years [5].
In particular, humans inhale about 53,700 particles of plastic a year and orally ingest anywhere between 74,000 and 121,000 annually [5]. Plastics production and environmental buildup are surging with modern prosperity and efficiency, posing a serious threat to human reproductive health as they accumulate in critical reproductive organs like the placenta.
Microplastics
“Microplastics could become the most dangerous environmental contamination of the 21st century, with plastic in everything we consume, it may seem helpless.” [18]
Microplastics are tiny particles of plastic that are contained in the air, plastic dust, food, fabrics, table salt, trash, and nearly every part of modern life. They can range from five millimeters to one micrometer (µm) [11]. Even smaller sizes of microplastics, called nanoplastics, pose a threat to human cells. Less than 100 nm in size, nanoplastics can cross all organs, including the placenta and blood system [11]. Microplastics of size ≤ 20 µm can enter any organ, and; ≤ 100 µm can be absorbed from the gut to the liver [11]. Scientists have discovered microplastics in many parts of the human body, including the liver, blood, and other reproductive organs, including the placenta [15].
Microplastics have multiple routes of getting into the body, which makes them a challenging threat for humans to overcome. To begin, they can be absorbed into the body by wearing clothes with fabrics containing plastic, like polyester. Although this most commonly occurs via inhalation of microplastics in the air, emerging theories also suggest that with long enough exposure to intact or open wounds, absorption of nanoplastics through the skin is possible as well. Inhalation can also occur from air pollution, specifically in areas with high carbon dioxide and dust levels.
In addition, microplastics can be consumed through foods we eat, or plastics we drink or touch, like plastic straws. Marine life also consumes a significant amount of microplastics from pollution in the ocean. Importantly for humans, this is an entry point to the food supply, as the contaminated marine life will then pass the microplastics up the food chain to humans when we eat seafood [11]. Moreover, cleaning products and cosmetics can contain a high amount of plastics that are absorbed into the skin [11]. Some estimates say that a credit card’s worth of microplastics is inhaled by an individual human every week [2].
A practical solution would be to pass the microplastics in the stool; however, the plastics do not always leave the body via waste. Sometimes, microplastics accumulate in the body over long periods of time and absorb into the intestines, bloodstream, and other tissues. Microplastics tend to find their way into crucial arteries and tissues due to their molecular composition.
They are made of synthetic polymers, a series of repeating monomers. The monomers in microplastics are made up of carbon and hydrogen atoms and occasionally have oxygen, nitrogen, chlorine, or sulfur atoms inside [3]. Some of the main components of microplastics are their polymer chains because, like polyethylene, they contain monomers like (–CH₂–CH₂–)ₙ [3]. Also, plastics usually contain additives to enhance their usual properties, but they also have harmful effects on humans. For example, phthalates, which make polyethylene flexible, negatively impact reproductive signals, while colorants are not chemically bonded to the polymer, and thus escape into the environment [3]. Most importantly, microplastics are mostly hydrophobic, which means they repel against water. This causes them to bind with oily substances and bioaccumulate in human tissues [3].
Female Reproductive System
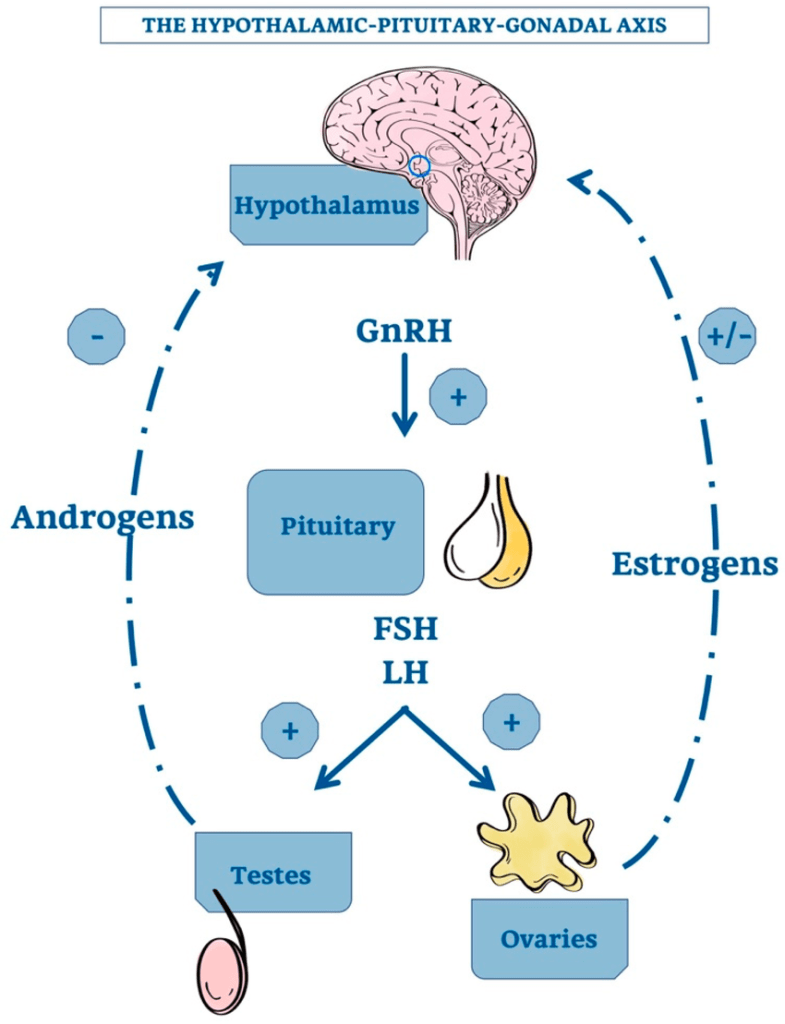
The reproductive system is a highly complex system requiring the coordination between several organ systems and the endocrine system to ensure the human body is an adequate environment for fetal development. The hypothalamic-pituitary-gonadal axis, located between the brain and reproductive organs helps to control ovulation and coordinate reproductive behavior [8].
First, a primary signal called the GnRH (gonadotropin-releasing hormone) is produced by the hypothalamic neurons, which stimulates the pituitary gland to release two important hormones: FSH (follicle–a fluid filled sac in the ovary that contains the immature egg–stimulating hormone) and LH (luteinizing hormone) [8]. These hormones lead to ovarian growth, egg maturation, and preparation of the uterine lining for pregnancy [8]. As the follicles grow, they start to make a form of estrogen known as estradiol, which will ultimately slow down the production of GnRH and FSH [8]. Once there is an adequate amount of estradiol, the GnRH and FSH will burst and surge, leading to ovulation. These reproductive hormones, such as GnRH, regulate the proper timing of a woman’s reproductive cycle [8].
However, foreign chemicals, microplastics, and agents can interfere with hormonal signals, either blocking or mimicking them. This disruption can cause infertility, irregular menstrual cycles, and complications in fetal development, since hormones are key to regulating and protecting the growth of vital organs like the baby’s brain and heart [8].
The placenta forms in a woman during pregnancy. The placenta is crucial for fetal development as it connects the fetal and maternal circulations via the umbilical cord. It supports the baby’s growth and development by providing nutrition and removing waste from the baby’s blood. In addition, the organ plays a major role in immunity because it helps the fetus identify self versus non-self cells and antigens. The placenta is located on the wall of the uterus lining and usually on the top, side, and sometimes even the lower area. When the placenta is too low, it raises a risk known as placenta previa, which is caused when the organ covers the cervical opening, and it can develop this way if microplastics were to block and change growth signaling for the placenta [14].
Microplastics in Female Reproduction
Microplastics enter the human placenta through many of the same pathways they use to accumulate in other tissues. First, they can be introduced through food consumption or inhalation [2]. Then, particles are absorbed through the gut and travel into the bloodstream, where they find their way into the placenta during pregnancy.
On a molecular level, after entering the body, their hydrophobic polymer chains prevent normal decomposition [2]. This means microplastics can proceed and bind to other toxins such as heavy metals, which can enhance the harmful effects in living organisms. Once inside the body, the microplastics can cross membranes such as those in the gut, like the M-cells in the intestinal lining, through the cellular process of endocytosis, which can take in foreign particles [2]. From there, they can enter the lymphatic system and/or the bloodstream [2].
Another pathway for microplastics is that sometimes they can bypass the digestive system completely through cells or between cells transport, which is also known as trans-cellular and paracellular transport [2]. Once in the bloodstream, microplastics can circulate to any part of the body, including the placenta. While the placenta does have a layer to protect it from harmful substances called a syncytiotrophoblast layer, nanoplastics can bypass this layer through endocytosis or passive diffusion through functional surfaces coated with proteins [2].
Once inside, the microplastics may interact with intracellular structures like the mitochondria, which can affect energy production, the endoplasmic reticulum, and as a result impact protein synthesis and lysosomes, ultimately leading to cell damage [2]. Studies show high levels of microplastics in human placental tissue:
In a 2024 study led by Dr. Matthew Campen and colleagues, microplastics were found in all 64 placentas studied, with amounts ranging from 6.5 to 790 micrograms per gram of tissue. Moreover, it was found that 54% of the plastic was polyethylene, the plastic that makes up plastic bags and bottles, with polyvinyl chloride and nylon being 10%, and the rest being nine other polymers [13]. This suggests that a majority of the placental microplastics are likely inhaled due to direct contact with the plastics on our mouth, nose, hands, etc.
Another study showed that 10.9% of all microplastics found in a human body were in the placenta, demonstrating how common microplastic exposure is during human development [5]. Thus, microplastics can enter the developing fetus through the placenta [13]. Multiple international studies have found microplastics within the placenta and neonatal samples, suggesting a widespread exposure of microplastics globally [4]. Between 2021 and 2023, seven studies were conducted in four countries, which showed a high percentage of microplastics in the placental tissue.
In 2021, an Italian study identified microplastics in four out of six placentas from vaginal births using light microscopy and Raman microspectroscopy [9]. In another Italian study, all ten placentas (from both vaginal and Cesarean section births) contained microplastics [9]. Electron microscopy revealed cellular damage, although the association with microplastics was not definitive [9]. Importantly, higher microplastics and polymer levels were linked to greater water consumption and frequent use of certain personal care products [9].
In 2022, an Iranian study detected microplastics in 13/13 placentas from the intrauterine growth restriction (IUGR) group and only 4/30 in the normal group [9]. This study implied that microplastic exposure may affect fetal development and normal growth. More studies also showed the presence of microplastics in cord blood samples [4]. However, only a few were tested since there is no commercially available test to find microplastics in placentas. These studies demonstrate that, as reproduction continues, this cycle could lead to a growing buildup of microplastics in future offspring and a possibility of new illnesses that will go unnoticed.
Placental microplastics affect reproduction and early fetal development. Fetal development begins from the first stage of pregnancy, often before many women realize they are pregnant [19]. There are three stages of fetal development: germinal, embryonic, and fetal [19]. The germinal stage is where the sperm and egg combine to form the zygote [19]. From there, the zygote turns into a blastocyst, where it is implanted into the uterus [19]. Next is the embryonic stage, usually from around the third week of pregnancy to the eighth week [19]. During this stage, the blastocyst becomes an embryo as the baby develops human characteristics such as organs [19]. At weeks five to six, the heart is recognized in the baby, and little arm and leg stubs are also discoverable [19]. Finally, the fetal stage begins around the ninth week and lasts until birth. During the fetal stage, the baby develops its primary sex characteristics that officially turn the embryo into a fetus. The fetus also grows hair and fingernails at this time and can start to move [19].
Microplastics can affect fetal development in several ways. Ultimately, babies are born pre-polluted [12].
“If we are seeing effects on placentas, then all mammalian life on this planet could be impacted,” says Dr. Matthew Campen, Regents’ Professor, UNM Department of Pharmaceutical Sciences.
Once the microplastics and nanoplastics enter cells, including both germ and somatic cells, they can cause oxidative damage, which can lead to DNA damage and cell death [16].
Microplastics can lead to cell death through pyroptosis [16], a highly inflammatory form of lytic programmed cell death caused by microbial infection [17]. When microplastics are detected, there is trafficking of immune cells like natural killer, T cells, and uterine dendritic cells to extinguish them as they are detected as non-self [16]. In mouse models, placental microplastics were shown to reduce the number of live births, alter the sex ratio of offspring, and cause fetal growth restriction, all effects that have also been observed in humans.
If one of these effects is already seen in humans, it raises the possibility that the others could follow. Since microplastics are present in human tissues, the outcomes seen in animal models like hormonal disruption, reduced sperm count and viability, decreased egg quality, neurophysiological and cognitive deficits, and disrupted embryonic development, [1] could also emerge in humans.
Furthermore, microplastics can change the gut microbiome and hormonal signaling, which can directly impact normal physiology and alter the signals sent between the uterus and embryo [1]. They do this by changing the balance and composition of the gut, which can lead to dysbiosis, an imbalance of the gut bacteria [10]. Some changes to the delicate gut microbiome could cause a condition called leaky gut, which shifts the previously semi-permeable membrane into a hyperpermeable one [10]. Emerging research demonstrates increasing rates of infertility, with scientists implicating environmental exposures, including microplastics.
Microplastics may also affect the endocrine system, which leads to neurodevelopmental issues in the offspring [1]. Another feature of abnormal pregnancies can be high blood pressure in mothers (like preeclampsia), which can result in organ failure and severe problems in the mother [1]. The endocrine system is the hormone-regulating system in your body that directly involves the glands of the gonads (ovaries and testes). Microplastics can interfere with the production of these hormones due to the additive factors the polymers carry, like Bisphenol A (BPA), which is used to harden the plastic [1].
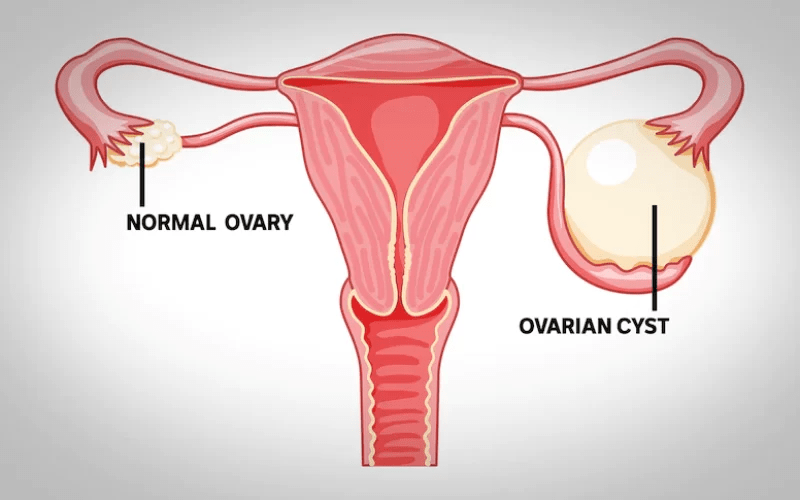
These chemicals are known as endocrine-disrupting chemicals. In addition to this, it can directly bind to the hormone receptors and block normal signaling [1]. Such effects can change gene expression, cause hormone-related cancers, and most importantly, impact fetal endocrine function and development, including lower birth weight and reproductive disorders [1]. Ovarian cysts—fluid-filled sacs that develop on or in the ovaries—can also be caused by microplastics in the reproductive system [15]. When a hormone signal is out of balance, it can trigger the egg not to be released, which can persist to form a cyst [15]. Although this is still being researched by scientists today, there has been a direct correlation in mice, suggesting microplastics disrupt ovarian follicle development.
While the immediate effects of microplastics in placentas are concerning, there are other long-term concerns, such as a generational impact, that raise a sense of urgency to the issue. First, microplastics do not disappear once a person dies [6]. The synthetic particles of microplastics resist biodegradation when the body is buried or even cremated [6]. This means it can reenter the ecosystem and harm other organisms [6]. On the other hand, microplastics are also being passed from generation to generation through parental gametes and the placenta. Microplastics can lead to more detrimental impacts that haven’t even been discovered yet. With more and more accumulation, the body can respond in many different ways that are hard to predict. However, it can be assumed that populations with more microplastics are more likely to be infertile in the future. One can imagine a scenario in which natural selection might occur, as people with less microplastics or who are less affected by their presence will be better able to survive and reproduce.
Summary and Conclusion
Microplastics lead to hormone imbalances of estrogen and other hormones in female bodies by disrupting hormone signaling (activating and blocking), and altering reproductive organ function and development, including infant birth weight, length, and head circumference [10]. Microplastics can interfere with gene expression or epigenetic markers, which can alter the way a fetus develops [10]. They can cut gene readings short, which could lead to affecting their length or head circumference [10]. Impaired egg development and follicular growth can impair fertility and have been linked with microplastic exposure [10]. Similarities can be seen in male fertility as microplastics affect the inflammatory response, change hormone levels with their disrupting and toxic chemicals, and cause cellular damage to the development of the gametes [5]. Overall, the effects of microplastics on reproductive systems have grave consequences, with evidence suggesting infertility in humans.
In addition to understanding the effects of microplastics on human health and reproduction, scientists are working to rid the body of microplastics. By studying plastic-eating microorganisms, they can examine the enzymes they have that allow them to process microplastics naturally [10]. Additionally, as there is increasing understanding of methods of exposure, such as inhalation or absorption, [10], there are ways to reduce the chance of microplastic exposure to your body. For example, humans face the biggest possibility of exposure from food. Fish is a great source of nutrients and protein, however, it is extremely crucial to know that fish carry large quantities of microplastics ingested in the ocean. By ensuring trash and plastics do not end up in aquatic ecosystems, humans can reduce the chance of microplastics entering the food chain. Scientists are also advocating for the elimination of single-use plastic and finding a more sustainable way to save the human population and the environment.
A Simple Technique for Studying the Interaction of Polypropylene-Based Microplastics with Adherent Mammalian Cells Using a Holder. Feb. 2025, research.ebsco.com/c/3uzxq3/search/details/hul46wuiu5?isDashboardExpanded=true&limiters=FT1%3AY&q=DE%20%22MICROPLASTICS%22.
Chemical Analysis of Microplastics and Nanoplastics: Challenges, Advanced Methods, and Perspectives. 26 Aug. 2021, pubs.acs.org/doi/10.1021/acs.chemrev.1c00178.
Cleveland Clinic. “Fetal Development.” Cleveland Clinic, 19 Mar. 2024, my.clevelandclinic.org/health/articles/7247-fetal-development-stages-of-growth.
Comparison of Microplastic Levels in Placenta and Cord Blood Samples of Pregnant Women With Fetal Growth Retardation and Healthy Pregnant Women. Kutahya Health Sciences University, 1 Apr. 2022. clinicaltrials.gov/study/NCT05070715?cond=placenta&term=microplastics&rank=1.
Exposure to Microplastics and Human Reproductive Outcomes: A Systematic Review. 29 Jan. 2024, obgyn.onlinelibrary.wiley.com/doi/10.1111/1471-0528.17756.
Haederle, Michael. “Microplastics in Every Human Placenta, New UNM Health Sciences Research Discovers.” UNM HSC Newsroom, 2024, hscnews.unm.edu/news/hsc-newsroom-post-microplastics.
Hunt K, Davies A, Fraser A, Burden C, Howell A, Buckley K, et al. Exposure to microplastics and human reproductive outcomes: A systematic review. BJOG. 2024; 131(5): 675–683. https://doi.org/10.1111/1471-0528.17756.
Leaky Gut Syndrome. Cleveland Clinic, 6 Apr. 2022, my.clevelandclinic.org/health/diseases/22724-leaky-gut-syndrome.
The United States is currently facing its greatest measles surge in almost thirty years, with 1200+ Americans testing positive for the disease so far this year. While some experts blame international travel, others believe vaccine hesitancy is the primary reason for this surge. However, to stay protected and stop the spread, we must first understand the science behind measles and what it takes to stay protected.
What is measles?
First documented in the early 12th century, measles ran rampant for centuries with hundreds of millions infected every year. An endemic disease, measles perpetually circulated and would flare up into cyclical outbreaks every 2-3 years. According to the National Library of Medicine,
“Measles […] caused more than 6 million deaths globally each year.”
To put this tremendous number into perspective, 6 million annual deaths is comparable to the population of the entire Dallas-Fort Worth metroplex getting wiped out every single year. Children under 15 were most vulnerable, and it was almost expectation that kids would experience the routine fever, cough, and blotchy rash before reaching adulthood.
How the Virus Spreads
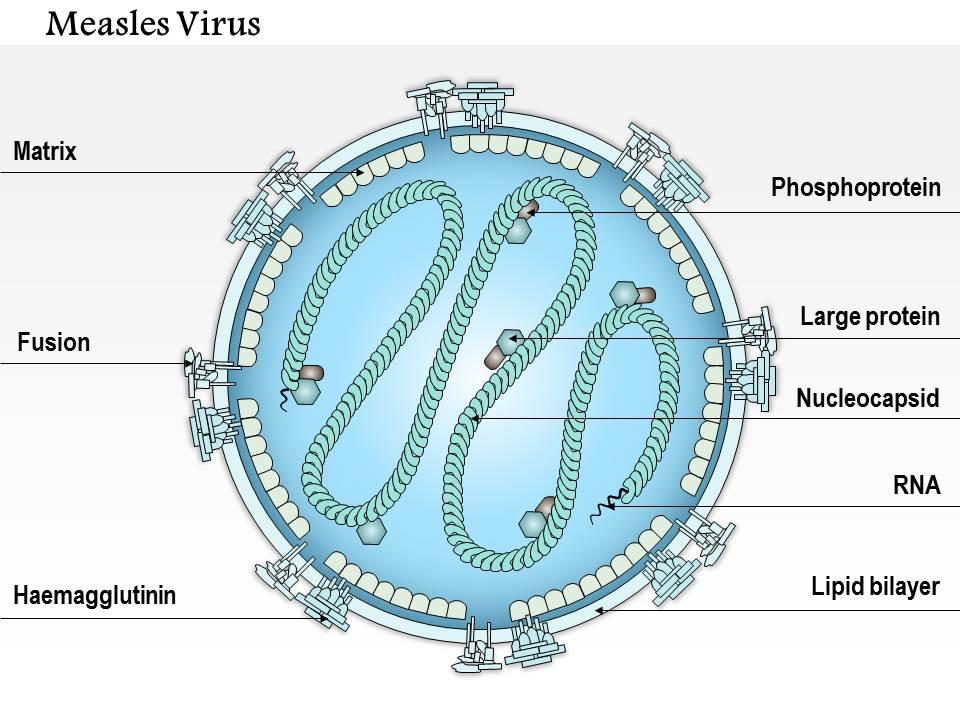
Often confused with smallpox and chickenpox, measles is an airborne pathogen that attacks cells in your respiratory tract as you breathe in the disease. The virus itself is composed of a single negative-sense RNA strand that is unreadable to human cells. However, measles carries a special enzyme that converts the previously unreadable virus into a positive-sense RNA, allowing proteins in our body to replicate and spread the disease.
The speed at which measles hijacks cells prevents the immune system from responding immediately, and groups measles together with other fast, aggressive negative-sense RNA viruses including influenza, rabies, and ebola.
Furthermore, measles is categorized as an enveloped virus. This means a lipid membrane envelops each cell and allows for easier access to infect healthy host cells. However, the measles virus exhibits one key vulnerability: soap and detergent can easily break down the fatty envelope, destroying its ability to infect.
Washing your hands and clothes significantly reduces the risk of virus from ever reaching your system, but remember, because measles is primarily airborne, sanitation does not completely prevent transmission.
How does the vaccine counteract the virus?
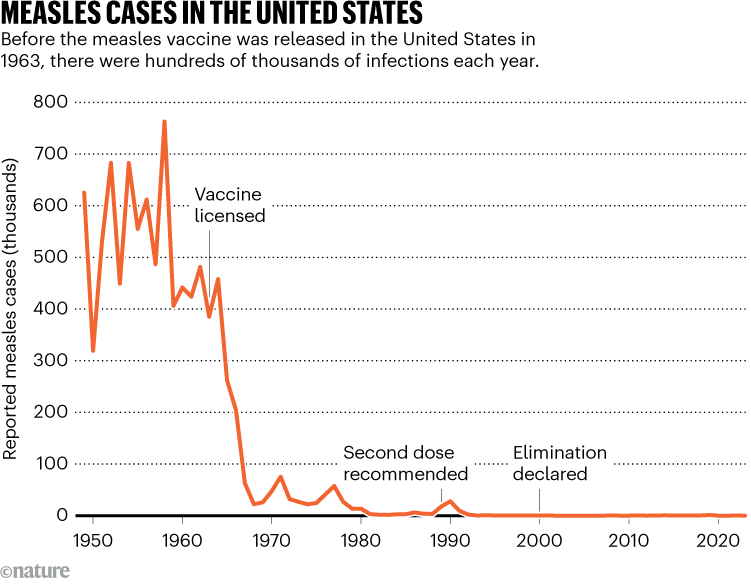
Though measles took the world by storm for centuries, in 1963 Dr. John Enders and his team developed the first measles vaccine. Often coined ‘the father of modern vaccines,’ Enders formulated the Edmonston-B strain, a killed virus vaccine.
The vaccine took the live measles virus and deactivated the disease’s genetic RNA so it could not reproduce, while preserving the outer proteins of the cell so the immune system could produce antibodies to combat the virus.
Despite its revolutionary effects, the Edmonston-B vaccination also presented major drawbacks. Immunity wore off over time, and people even developed ‘atypical measles,’ a form of measles with heightened symptoms including higher fevers, pneumonitis, and pain not typical of regular measles.
Therefore, 5 years after the initial Edmonston-B strain was drafted, in 1968 microbiologist Dr. Maurice Hilleman developed the Edmonston-Enders strain. This vaccine used an attenuated form of the 1963 Edmonston-B strain, by allowing the virus to grow in chick embryos, first. As the measles virus mutated to survive in chick cells, it slowly lost the ability to cause full-blown disease in human cells.
The final product? A live virus that infected your cells enough to train your immune system, but not enough to cause the atypical disease and heightened side-effects of the 1963 Edmonston-B strain.
A few years later, the MMR vaccine was created, combining defense against measles, mumps, and rubella in one shot. Two doses produced a 97% chance of protection against the diseases. Today, it is still recommended that children take two doses of the MMR vaccine; one dose as an infant, and another between 4 and 6 years old.
So why is there suddenly a spike in US measles cases?
As I write this article, there have been 1227 confirmed measles cases so far this year, with the biggest outbreak taking place in West Texas. There, 97 people have contracted the disease with two unvaccinated children dying, the first measles-related deaths in the US since 2015.
Overall, this spike in cases is accredited to decreased vaccination rates since the COVID-19 pandemic. According to John Hopkins University,
“Out of 2,066 studied [U.S.] counties, [in] 1,614 counties, 78%, reported drops in vaccinations and the average county-level vaccination rate fell 93.92% pre-pandemic to 91.26% post-pandemic-an average decline of 2.67%, moving further away from the 95% herd immunity threshold to predict or limit the spread of measles.”
During the COVID-19 pandemic, public health staff were pulled from routine duties like immunizations to focus on COVID testing, contact tracing, and hospital coordination. According to UNICEF USA,
“As access to health services and immunization outreach were curtailed [due to the pandemic], the number of children not receiving even their very first vaccinations increased in all regions. As compared with 2019, […] 3 million more children missed their first measles dose.”
Centers for Disease Control and Prevention / New York Times
Going forward, efforts to close the immunity gap will depend on identifying under-vaccinated populations and ensuring routine and follow-up vaccinations. As more people understand measles transmission and how the vaccine works, we will be better equipped to respond, and the risk of future outbreaks can be reduced significantly.
Gastañaduy, P. A., Goodson, J. L., Panagiotakopoulos, L., Rota, P. A., Orenstein, W. A., & Patel, M. (2021, September 30). Measles in the 21st century: Progress toward achieving and sustaining elimination. The Journal of infectious diseases. https://pmc.ncbi.nlm.nih.gov/articles/PMC8482021/
Sabsay, K. R., & Te Velthuis, A. J. W. (2023, December 20). Negative and ambisense RNA virus ribonucleocapsids: More than protective armor. Microbiology and molecular biology reviews : MMBR. https://pmc.ncbi.nlm.nih.gov/articles/PMC10732063/